Coronary artery aneurysms (CAAs) are defined as a dilation of 1.5 times the diameter of a normal adjacent coronary artery, and CAAs larger than 20 cm are classified as giant. CAAs are typically asymptomatic, but complications can be fatal. There is currently no consensus on treatment, although medical, percutaneous, and surgical options have all been previously described in the literature. Additionally, there is little published video footage of the surgical exclusion of giant coronary artery aneurysms. This report describes the case of a 53-year-old man with a persistent globus sensation who was found to have a 4.5 cm right coronary artery aneurysm with diffuse calcification of the right coronary artery. He underwent exclusion of the aneurysm and coronary artery bypass grafting (radial artery to the right coronary artery and left internal mammary artery to the left anterior descending artery). Due to heavy calcification in the vessel wall, the right coronary artery both proximal and distal to the aneurysm was ligated with a pericardial buttress. The patient had no major adverse events and was discharged six days after surgery. This report includes detailed video footage of the giant coronary artery aneurysm exclusion technique. This case and accompanying video footage will help prepare surgeons to manage adult patients with CAAs and diffuse coronary atherosclerosis.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 10, Issue 4) |
| DOI | 10.11648/j.ijcts.20241004.12 |
| Page(s) | 56-61 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Giant Coronary Artery Aneurysm, Right Coronary Artery, Bypass Grafting, Arterial Grafts
CAA | Coronary Artery Aneurysm |
CT | Computed Tomography |
CTA | Computed Tomography Angiography |
ED | Emergency Department |
LAD | Left Anterior Descending Artery |
LIMA | Left Internal Mammary Artery |
PCI | Percutaneous Coronary Intervention |
RCA | Right Coronary Artery |
Below is the link to the supplementary material:
| [1] | Dimagli A, Malas J, Chen S, et al. Coronary Artery Aneurysms, Arteriovenous Malformations, and Spontaneous Dissections-A Review of the Evidence. Ann Thorac Surg. 2024; 117(5): 887-896. |
| [2] | Luo Y, Tang J, Liu X, et al. Coronary Artery Aneurysm Differs From Coronary Artery Ectasia: Angiographic Characteristics and Cardiovascular Risk Factor Analysis in Patients Referred for Coronary Angiography. Angiology. 2017; 68(9): 823-830. |
| [3] | Sheikh AS, Hailan A, Kinnaird T, et al. Coronary Artery Aneurysm: Evaluation, Prognosis, and Proposed Treatment Strategies. Heart Views. 2019; 20(3): 101-108. |
| [4] | Mrdović I, Jozić T, Asanin M, et al. Myocardial reinfarction in a patient with coronary ectasia. Cardiology. 2004; 102(1): 32-34. |
| [5] | Topaz O, Rutherford MS, Mackey-Bojack S, et al. Giant aneurysms of coronary arteries and saphenous vein grafts: angiographic findings and histopathological correlates. Cardiovasc Pathol. 2005; 14(6): 298-302. |
| [6] | Li D, Wu Q, Sun L, et al. Surgical treatment of giant coronary artery aneurysm. The Journal of Thoracic and Cardiovascular Surgery. 2005; 130(3): 817-21. |
| [7] | Pham V, De Hemptinne Q, Grinda JM, et al. Giant coronary aneurysms, from diagnosis to treatment: a literature review. Archives of cardiovascular diseases. 2020; 113(1): 59-69. |
| [8] | Ghazinour M, Ghaedi A, Bazrgar A, et al. A huge coronary artery aneurysm with ST-elevation myocardial infarction: A case report and review of literature. Heliyon. 2024; 10(19). |
| [9] | Mossberg M, Mohammad AJ, Kahn F, et al. High risk of coronary artery aneurysm in Kawasaki disease. Rheumatology. 2021; 60(4): 1910-4. |
| [10] | Bararu-Bojan I, Badulescu OV, Badescu MC, et al. New Insights into the Pathophysiology of Coronary Artery Aneurysms. Diagnostics. 2024; 14(19): 2167. |
| [11] | Chalikias G, Tsigalou C, Stakos D, et al. Coronary artery ectasia as an autoimmune disease paradigm in a cross-sectional case-control study. The American Journal of Cardiology. 2023; 205: 63-8. |
| [12] | Joo HJ, Woong Yu C, Choi R, et al. Clinical outcomes of patients with coronary artery aneurysm after the first generation drug‐eluting stent implantation. Catheterization and Cardiovascular Interventions. 2018; 92(3): E235-45. |
| [13] | Nichols L, Lagana S, Parwani A. Coronary artery aneurysm: a review and hypothesis regarding etiology. Archives of pathology & laboratory medicine. 2008; 132(5): 823-8. |
| [14] | Forte E, Aiello M, Inglese M, et al. Coronary artery aneurysms detected by computed tomography coronary angiography. European Heart Journal-Cardiovascular Imaging. 2017; 18(11): 1229-35. |
| [15] | Cohen P, O'Gara PT. Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiology in review. 2008; 16(6): 301-4. |
| [16] | Vadalà G, Di Caccamo L, Alaimo C, et al. Coronary Arteries Aneurysms: A Case-Based Literature Review. Diagnostics (Basel). 2022; 12(10): 2534. |
| [17] | Boyer N, Gupta R, Schevchuck A, et al. Coronary artery aneurysms in acute coronary syndrome: case series, review, and proposed management strategy. The Journal of Invasive Cardiology. 2014; 26(6): 283-90. |
| [18] | Khubber S, Chana R, Meenakshisundaram C, et al. Coronary artery aneurysms: outcomes following medical, percutaneous interventional and surgical management. Open Heart. 2021; 8(1): e001440. |
| [19] | Lee MG, Lefkovits J, Joshi SB, et al. Multi-vessel giant coronary artery aneurysms: An unusual cause of chest pain. Radiology Case Reports. 2023; 18(3): 814-7. |
| [20] | Veenu J, Shetty GG, Adhyapak SM, et al. Giant coronary artery aneurysms involving all three coronary arteries. indian heart journal. 2014; 66(6): 727-30. |
| [21] | Della Rosa F, de Nicolas JM, Bonfils L, et al. Symptomatic giant coronary artery aneurysm treated with covered stents. Coronary Artery Disease. 2020; 31(7): 658-9. |
| [22] | Crawley PD, Mahlow WJ, Huntsinger DR, et al. Giant coronary artery aneurysms: review and update. Texas Heart Institute Journal. 2014; 41(6): 603-8. |
| [23] | Konen E, Feinberg MS, Morag B, et al. Giant right coronary aneurysm-CT angiographic and echocardiographic findings. AJR. 2001; 177: 689-91. |
| [24] | Hao WR, Chen FC, Kao PF, et al. Adult giant coronary artery aneurysm-a case report and literature review. Acta Cardiol Sin. 2004; 20: 187-90. |
| [25] | Grandmougin D, Croisille P, Robin C, et al. Giant coronary aneurysm mimicking a compressive cardiac tumor: imaging features and operative strategy. Cardiovasc Pathol. 2005; 14 (5): 272-5. |
| [26] | McGlinchey PG, Maynard SJ, Graham AN, et al. Giant aneurysm of the right coronary artery compressing the right heart. Circulation. 2005; 112: e66-e67. |
| [27] | Augustin N, Wessely R, Porner M, et al. Giant coronary aneurysm obstructing the right heart. Lancet. 2006; 368 (9533): 386. |
| [28] | Kumar G, Karon BL, Edwards WD, et al. Giant coronary artery aneurysm causing superior vena cava syndrome and congestive heart failure. Am J Cardiol. 2006; 98: 986-88. |
| [29] | Takano MI, Oikawa M, Yamaki T, et al. A case of recurrent myocardial infarction caused by a giant right coronary artery aneurysm. J Am Soc Echocardiogr. 2007; 20 (11): 1318. e5-1318. e8. |
| [30] | Altarabsheh SE, Deo SV, Rababa'h A, et al. Giant right coronary artery aneurysm in the setting of the acute coronary syndrome: A case report. Journal of Cardiac Surgery. 2020; 35(9): 2379-81. |
| [31] | Collins P, Webb CM, Chong CF, et al. Radial artery versus saphenous vein patency randomized trial: five-year angiographic follow-up. Circulation. 2008; 117(22): 2859-64. |
| [32] | Gaudino M, Benedetto U, Fremes S, et al. Radial-artery or saphenous-vein grafts in coronary-artery bypass surgery. New England Journal of Medicine. 2018; 378(22): 2069-77. |
APA Style
Mullis, D. M., Alnasir, D., Garrison, A., Vargas, N. M., Tsai, L., et al. (2024). Exclusion of a Giant Right Coronary Artery Aneurysm with Concomitant Bypass Grafting. International Journal of Cardiovascular and Thoracic Surgery, 10(4), 56-61. https://doi.org/10.11648/j.ijcts.20241004.12
ACS Style
Mullis, D. M.; Alnasir, D.; Garrison, A.; Vargas, N. M.; Tsai, L., et al. Exclusion of a Giant Right Coronary Artery Aneurysm with Concomitant Bypass Grafting. Int. J. Cardiovasc. Thorac. Surg. 2024, 10(4), 56-61. doi: 10.11648/j.ijcts.20241004.12
AMA Style
Mullis DM, Alnasir D, Garrison A, Vargas NM, Tsai L, et al. Exclusion of a Giant Right Coronary Artery Aneurysm with Concomitant Bypass Grafting. Int J Cardiovasc Thorac Surg. 2024;10(4):56-61. doi: 10.11648/j.ijcts.20241004.12
@article{10.11648/j.ijcts.20241004.12,
author = {Danielle Maria Mullis and Daniel Alnasir and Alyssa Garrison and Nataly Montano Vargas and Lillian Tsai and John Ward MacArthur},
title = {Exclusion of a Giant Right Coronary Artery Aneurysm with Concomitant Bypass Grafting
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {10},
number = {4},
pages = {56-61},
doi = {10.11648/j.ijcts.20241004.12},
url = {https://doi.org/10.11648/j.ijcts.20241004.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20241004.12},
abstract = {Coronary artery aneurysms (CAAs) are defined as a dilation of 1.5 times the diameter of a normal adjacent coronary artery, and CAAs larger than 20 cm are classified as giant. CAAs are typically asymptomatic, but complications can be fatal. There is currently no consensus on treatment, although medical, percutaneous, and surgical options have all been previously described in the literature. Additionally, there is little published video footage of the surgical exclusion of giant coronary artery aneurysms. This report describes the case of a 53-year-old man with a persistent globus sensation who was found to have a 4.5 cm right coronary artery aneurysm with diffuse calcification of the right coronary artery. He underwent exclusion of the aneurysm and coronary artery bypass grafting (radial artery to the right coronary artery and left internal mammary artery to the left anterior descending artery). Due to heavy calcification in the vessel wall, the right coronary artery both proximal and distal to the aneurysm was ligated with a pericardial buttress. The patient had no major adverse events and was discharged six days after surgery. This report includes detailed video footage of the giant coronary artery aneurysm exclusion technique. This case and accompanying video footage will help prepare surgeons to manage adult patients with CAAs and diffuse coronary atherosclerosis.
},
year = {2024}
}
TY - JOUR T1 - Exclusion of a Giant Right Coronary Artery Aneurysm with Concomitant Bypass Grafting AU - Danielle Maria Mullis AU - Daniel Alnasir AU - Alyssa Garrison AU - Nataly Montano Vargas AU - Lillian Tsai AU - John Ward MacArthur Y1 - 2024/11/28 PY - 2024 N1 - https://doi.org/10.11648/j.ijcts.20241004.12 DO - 10.11648/j.ijcts.20241004.12 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 56 EP - 61 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20241004.12 AB - Coronary artery aneurysms (CAAs) are defined as a dilation of 1.5 times the diameter of a normal adjacent coronary artery, and CAAs larger than 20 cm are classified as giant. CAAs are typically asymptomatic, but complications can be fatal. There is currently no consensus on treatment, although medical, percutaneous, and surgical options have all been previously described in the literature. Additionally, there is little published video footage of the surgical exclusion of giant coronary artery aneurysms. This report describes the case of a 53-year-old man with a persistent globus sensation who was found to have a 4.5 cm right coronary artery aneurysm with diffuse calcification of the right coronary artery. He underwent exclusion of the aneurysm and coronary artery bypass grafting (radial artery to the right coronary artery and left internal mammary artery to the left anterior descending artery). Due to heavy calcification in the vessel wall, the right coronary artery both proximal and distal to the aneurysm was ligated with a pericardial buttress. The patient had no major adverse events and was discharged six days after surgery. This report includes detailed video footage of the giant coronary artery aneurysm exclusion technique. This case and accompanying video footage will help prepare surgeons to manage adult patients with CAAs and diffuse coronary atherosclerosis. VL - 10 IS - 4 ER -
Department of Cardiothoracic Surgery, Stanford University, Stanford, USA
Biography: Danielle Mullis is a medical student at Stanford University. She completed her undergraduate studies at the University of Michigan, where she majored in Biomolecular Sciences and Spanish. She worked for two years as an Emergency Medical Technician and MCAT teacher, while also doing inorganic chemistry research in the Szymczak Lab. At Stanford University, she is a Cardiovascular Interest Group Leader, CVI Early Career Committee member, and Cardinal Free Clinic volunteer. She is part of the Physician Scientist Training Program, where she dedicated an additional year to research in the Dr. Joseph Woo Lab during medical school. She is passionate about cardiac surgery and research.

Department of Cardiothoracic Surgery, Stanford University, Stanford, USA
Department of Cardiothoracic Surgery, Stanford University, Stanford, USA
Department of Cardiothoracic Surgery, Stanford University, Stanford, USA
Department of Cardiothoracic Surgery, Stanford University, Stanford, USA
Department of Cardiothoracic Surgery, Stanford University, Stanford, USA

Figure 1. Pre-Operative Imaging of a Giant Right Coronary Artery Aneurysm. A) 4.5 cm right coronary artery aneurysm (white arrow) seen on chest computed tomography. B) Giant right coronary artery aneurysm noted on cardiac catheterization.
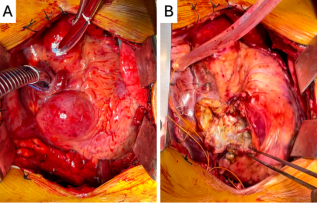
Figure 2. Giant Right Coronary Artery Aneurysm with Coronary Artery Bypass Grafting. A) Intraoperative photograph of the giant right coronary artery aneurysm at the start of the case. B) Intraoperative photograph after exclusion and bypass grafting.
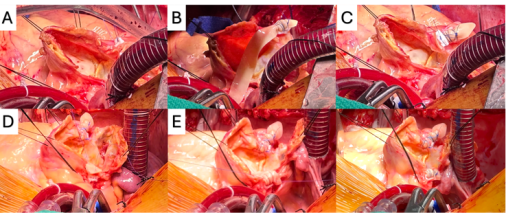
Figure 3. Intraoperative Photographs of the Giant Coronary Artery Aneurysm Exclusion. A) The aneurysm sac was opened longitudinally. B) Pledgets and pericardium were used to ligate the distal right coronary artery (RCA). C) The distal RCA was ligated with a pericardial buttress. D) An arteriotomy was made distal to the ligated RCA, and an end-to-side anastomosis was performed between the radial artery graft and the RCA. E) Pledgets and pericardium were used to ligate the proximal RCA. F) Intraoperative photograph of the aneurysm at the end of the case.

