One of the main therapeutic options for the treatment of peripheral arterial disease is endovascular treatment, which has proven to be an effective and less invasive alternative to open surgery. This approach offers several advantages, such as faster recovery and a shorter hospital stay. However, it can also lead to complications, including restenosis and in-stent occlusion, which can compromise the effectiveness of the procedure and have a negative impact on patients' quality of life. Faced with this problem, innovative solutions have emerged, such as rotational atherectomy with the BYCROSS® device, which has positioned itself as a promising tool for the treatment of complex arterial lesions and in-stent thrombosis. This device allows controlled removal of obstructive material, optimizes blood flow and improves short- and long-term outcomes. In this case report, we present a patient with a history of peripheral arterial disease who developed in-stent thrombosis, a common but difficult complication associated with previous endovascular treatments. The patient was successfully treated with rotational atherectomy using the BYCROSS® device, achieving excellent angiographic and clinical results. Subsequently, a significant improvement in symptoms and quality of life was observed. This case highlights the importance of innovative technologies in current clinical practice and the need for a comprehensive and personalized approach in the treatment of vascular complications in patients with peripheral arterial disease.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Peripheral arterial occlusive disease (PAD) is a condition that is increasingly prevalent in our society and represents a major challenge for healthcare systems
[1]
Bisdas T, Borowski M, Stavroulakis K et al. Endovascular therapy versus bypass surgery as first-line treatment strategies for critical limb ischemia: results of the interim analysis of the CRITISCH registry. JACC Cardiovasc Interv. 2016; 9: 2557–2565.
One of the most common treatment options for PAD is endovascular treatment, which is effective but can lead to complications such as restenosis or in-stent occlusion. These complications are often caused by intimal hyperplasia or stent thrombosis
[3]
Giannopoulos S, Kokkinidis DG, Jawaid O, Behan S, Hossain P, Alvandi B, Foley TR, Singh GD, Waldo SW, Armstrong EJ. Turbo-Power™ Laser Atherectomy Combined with Drug-coated Balloon Angioplasty is Associated with Improved One-Year Outcomes for the Treatment of Tosaka II and III Femoropopliteal In-stent Restenosis. Cardiovasc Revasc Med. 2020; 21(6): 771-778.
, which can compromise the success of the initial treatment.
In response to these challenges, innovations in the field of vascular medicine have emerged in recent years, such as devices for retarding rotating atherectomy. An outstanding example is the BYCROSS® device (Taryag Medical Ltd., Or Akiva, Israel), which has proven to be a valuable tool in the treatment of stent thrombosis. This device combines low-speed thrombectomy with a variable tip diameter and high aspiration capacity, allowing effective clot removal. Thanks to its design, the risk of embolization is reduced to a minimum, making it a safe and effective option for patients
[4]
Tessarek J, Kolvenbach R. Safety and effectiveness of bycross rotational atherectomy and aspiration device: a prospective, multi-center pre-market approval study. CVIR Endovasc. 2023; 29; 6(1): 19.
. The main disadvantage of using these devices is distal embolization2 and, more rarely, rupture of the treated artery.
Ethical Approval and Informed Consent
Ethical approval was not required as all data was anonymized. Informed consent was obtained from the patient. The patient consented to the description of his clinical course for educational purposes.
2. Case Report
We present the case of a 70-year-old female patient, ex-smoker, diabetic and hypertensive, who underwent coronary stent implantation 5 years ago due to ischemic heart disease. She came to the emergency room because a lesion had occurred in the pretibial area of the right lower extremity after a trauma.
On clinical examination, she was hemodynamically stable, afebrile and in good general condition. On vascular examination, the carotid pulses and the pulses in the upper limbs were present. However, left femoro-popliteal obliteration was observed in the lower limbs and no pulse was present in the right lower limb where she had a pretibial ulcer with necrotic margins and signs of infection.
CT angiography of the lower extremities is requested, which shows patency of the right iliac axis, occlusion of the right common femoral artery with patency of the deep femoral artery. At the level of the right femoro-popliteal axis, an occlusion of the superficial femoral artery is observed at the level of the adductor canal, which repermeabilizes in the second part of the popliteal artery and keeps this and the three distal vessels patency.
The procedure includes thromboendarterectomy of the common femoral artery and the origin of the superficial femoral artery, closure with a bovine pericardial patch and implantation of two uncovered SuperaTM stents from the second part of the popliteal artery to the middle third of the superficial femoral artery in the right lower limb.
The patient is doing well postoperatively, the foot and posterior tibial pulses are present again. The patient is discharged from hospital. One month after surgery, the patient begins experiencing acute pain in the right foot and presents to the emergency room with erythrosis of the entire foot.
Upon vascular examination, carotid pulses are maintained. In the upper extremities, in the left lower extremity, the already known femoropopliteal obliteration, and in the right lower extremity, the popliteal and distal pulses have been lost, maintaining the femoral pulse lesion in the right pretibial region with good progress and healing.
Arterial Doppler ultrasound was performed on the right lower extremity with common femoral artery patency and occlusion of the SuperaTM stent, and the third portion of the popliteal artery was patent with a monophasic curve.
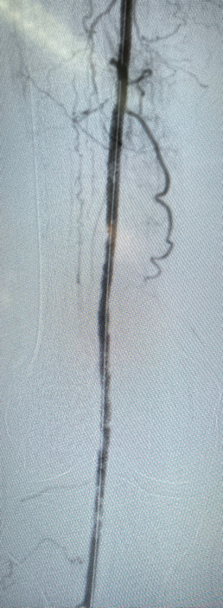
Endovascular rescue of thrombosed stents is decided in the operating room through an antegrade ultrasound-guided puncture in the superficial femoral artery, avoiding puncturing the bovine pericardium patch in the right groin. A short 7F introducer is placed, and arteriography is performed (Figure 1), where the occlusion of the stents from the middle third of the superficial femoral artery to the second portion of the popliteal artery is confirmed.
Figure 1. Initial arteriography with stent occlusion and development of collateral circulation. Patency of the third part of the popliteal artery.
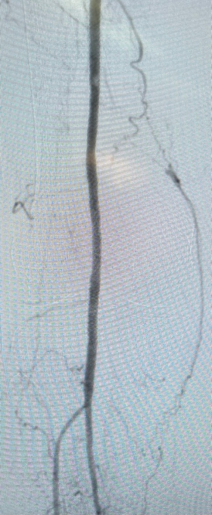
We proceed with the Glidewire Advantaje® guidewire from Terumo 0.035 to the peroneal artery with the help of a Berestein catheter. Exchange of a short 7F introducer for a 7F introducer of 45 cm in length and through this, the 70 cm BYCROSS® device. Several passes are made with and without the wings, thromboaspirating a large part of the thrombus as shown in Figure 2.
Figure 2. Arteriography after thromboaspiration with the BYCROSS® device.
Finally, the treated area is angioplastied with drug-eluting balloon stents. It is obtaining a good angiographic result as seen in figure 3. The closure is performed using a percutaneous device that is effective. During the procedure, 3000 IU of sodium enoxaparin is administered and 70 cc of iodinated contrast diluted to 50% with saline are used.
Figure 3. Final arteriography showing the patency of the stents, the anterior tibial artery and the tibioperoneal trunk.
The patient recovers posterior tibial and right pedal pulses, being discharged 24 hours after the procedure with rivaroxaban 2.5 mg and acetylsalicylic acid 100 mg, which will be maintained for 6 months, after which she will continue with simple lifelong antiplatelet therapy. In the monthly follow-up consultation, the pulses are stable, and the lesion is showing good progress.
3. Discussion
Since the commercialization of the BYCROSS® device, various studies have been conducted that demonstrate its effectiveness as an atherectomy tool, especially in the treatment of peripheral artery disease. (EAP). Research conducted by Tessarek
[4]
Tessarek J, Kolvenbach R. Safety and effectiveness of bycross rotational atherectomy and aspiration device: a prospective, multi-center pre-market approval study. CVIR Endovasc. 2023; 29; 6(1): 19.
has highlighted the benefits of this device in improving arterial flow and reducing complications associated with endovascular procedures. However, it is important to note that there is a lack of literature specifically addressing the outcomes obtained with rotational atherectomy devices in cases of thrombotic occlusions of implanted stents, particularly in situations of chronic occlusions in the superficial femoral and popliteal arteries.
A relevant study conducted by Pan
[6]
Pan T, Tian SY, Liu Z, Zhang T, Li C, Ji DH. Combination of RotarexⓇS Rotational Atherothrombectomy and Drug-Coated Balloonangioplasty for Femoropopliteal Total In-Stent Occlusion. Ann Vasc Surg. 2022; 80: 213-22.
has yielded significant results in evaluating the use of rotational atherectomy in patients with stent thrombosis in femoropopliteal pathology. This study concludes that the combination of rotational atherectomy and drug-eluting angioplasty is a safe and effective approach for treating total in-stent femoropopliteal occlusions, showing positive results during a 12-month follow-up. When comparing the combined treatment with drug-eluting angioplasty alone, a notable difference was observed in the rates of rescue stent placement: 22.9% in the group treated with atherectomy plus angioplasty versus 59.0% in the group that received only angioplasty (P = 0.01). Additionally, the Kaplan-Meier analysis revealed an estimated primary patency rate of 82.0 ± 6.7% for the group that received rotational atherectomy along with angioplasty, while the group treated only with angioplasty showed a significantly lower rate of 60.9 ± 8.3% (P = 0.04)
[7]
Fan W, Lu S, Tan J, Cui X, Liang K, Zhu L, He Q, Yu B, Shi W. Midterm Results of Drug-Coated Balloon Alone or Combined with Rotarex Thrombectomy Device for Treatment of Subacute Femoropopliteal Artery Thrombotic Occlusion. Ann Vasc Surg. 2023; 92: 240-8.
Similar results were reported by other researchers such as Wang
[8]
Wang Q, Zhu RM, Ren HL, Leng R, Zhang WD, Li CM. Combination of Percutaneous Rotational Thrombectomy and Drug-Coated Balloon for Treatment of Femoropopliteal Artery Nonembolic Occlusion: 12-Month Follow-up. J Vasc Interv Radiol. 2020; 31(10): 1661-7.
Liao CJ, Song SH, Li T, Zhang Y, Zhang WD. Combination of Rotarex Thrombectomy and Drug-Coated Balloon for the Treatment of Femoropopliteal Artery In-Stent Restenosis. Ann Vasc Surg. 2019; 60: 301-7.
, who also concluded that the combined treatment of rotational atherectomy and drug-eluting angioplasty outperforms angioplasty alone in cases of thrombosis of stents implanted in the femoropopliteal axis. For its part, Rodoplu
[10]
Rodoplu O, Oztas DM, Meric M, Beyaz MO, Ulukan MO, Yildiz CE, Unal O, Ugurlucan M. Efficacy of Rotational Atherectomy Followed by Drug-coated Balloon Angioplasty for the Treatment of Femoropopliteal Lesions-Comparison with Sole Drug-coated Balloon Revascularization: Two-year Outcomes. Ann Vasc Surg. 2021; 73: 222-33.
obtained even more encouraging findings by demonstrating the combination of rotational atherectomy and drug-eluting angioplasty. In their study, a notable difference in the rates of stent implantation necessity was observed between the two treated groups. Specifically, the group that received the combination of rotational atherectomy and angioplasty showed a stent implantation rate of 5.1%, compared to 20.6% in the group that was treated solely with drug-eluting angioplasty (p < 0.001), concluding that this combination is safe and effective.
As far as the comparison between rotational atherectomy and classic bypass is concerned, there are not enough studies on this topic. However, Tebarek
[11]
Teßarek J, Elger F, Kolvenbach R, Liebetrau D. Atherektomie mit einem neuen System, das noch mehr kann [Atherectomy with a Novel Device Offering Wider Options]. Zentralbl Chir. 2023 Oct; 148(5): 429-437. German.
suggests in his study that the BYCROSS® device is an effective and safe alternative to bypass, but that further studies are needed. Although antegrade access via the common femoral artery is most commonly used, there is also the possibility of retrograde access via the popliteal artery, depending on the type of lesion, as described by Tanyeli
[12]
Tanyeli O, Guner A, Yildirim S, Gunerhan Y, Isik M. Efficacy of the retrograde popliteal artery approach and results of rotational atherothrombectomy in total sfa occlusion. Turk J Vasc Surg. Published online November 27, 2024.
To date, the BYCROSS® device has been used in our center in a total of 2 patients in combination with medical angioplasty. Excellent results were achieved, both distal pulses were restored, and primary patency was 100% in the first 3 months. We will continue the follow-up to investigate this patency in the long term and to increase our sample size with additional patients.
4. Conclusion
The combination of rotational atherectomy with the BYCROSS® device and medical angioplasty represents an effective and safe therapeutic option for the treatment of in-stent thrombosis in the femoro-popliteal axis, particularly in patients with peripheral arterial occlusive disease. As this technique is minimally invasive, it allows for faster recovery and earlier discharge from the hospital, resulting in a significant reduction in the patient's hospital stay and recovery time.
Although the current results are promising, long-term studies are needed to assess the durability of the patency of the treated lesions and to make more accurate comparisons with open surgery. These studies will make it possible to consolidate the efficacy of this technique and determine its definitive role in the treatment of in-stent thrombosis in clinical practice.
Abbreviations
PAD
Peripheral Arterial Occlusive Disease
Author Contributions
Antonio García de Vargas: Conceptualization, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing
The authors declare that they have no conflicts of interest.
References
[1]
Bisdas T, Borowski M, Stavroulakis K et al. Endovascular therapy versus bypass surgery as first-line treatment strategies for critical limb ischemia: results of the interim analysis of the CRITISCH registry. JACC Cardiovasc Interv. 2016; 9: 2557–2565.
Pan T, Tian SY, Liu Z, Zhang T, Li C, Ji DH. Combination of RotarexⓇS Rotational Atherothrombectomy and Drug-Coated Balloonangioplasty for Femoropopliteal Total In-Stent Occlusion. Ann Vasc Surg. 2022; 80: 213-22.
Fan W, Lu S, Tan J, Cui X, Liang K, Zhu L, He Q, Yu B, Shi W. Midterm Results of Drug-Coated Balloon Alone or Combined with Rotarex Thrombectomy Device for Treatment of Subacute Femoropopliteal Artery Thrombotic Occlusion. Ann Vasc Surg. 2023; 92: 240-8.
Wang Q, Zhu RM, Ren HL, Leng R, Zhang WD, Li CM. Combination of Percutaneous Rotational Thrombectomy and Drug-Coated Balloon for Treatment of Femoropopliteal Artery Nonembolic Occlusion: 12-Month Follow-up. J Vasc Interv Radiol. 2020; 31(10): 1661-7.
Liao CJ, Song SH, Li T, Zhang Y, Zhang WD. Combination of Rotarex Thrombectomy and Drug-Coated Balloon for the Treatment of Femoropopliteal Artery In-Stent Restenosis. Ann Vasc Surg. 2019; 60: 301-7.
Rodoplu O, Oztas DM, Meric M, Beyaz MO, Ulukan MO, Yildiz CE, Unal O, Ugurlucan M. Efficacy of Rotational Atherectomy Followed by Drug-coated Balloon Angioplasty for the Treatment of Femoropopliteal Lesions-Comparison with Sole Drug-coated Balloon Revascularization: Two-year Outcomes. Ann Vasc Surg. 2021; 73: 222-33.
Teßarek J, Elger F, Kolvenbach R, Liebetrau D. Atherektomie mit einem neuen System, das noch mehr kann [Atherectomy with a Novel Device Offering Wider Options]. Zentralbl Chir. 2023 Oct; 148(5): 429-437. German.
Tanyeli O, Guner A, Yildirim S, Gunerhan Y, Isik M. Efficacy of the retrograde popliteal artery approach and results of rotational atherothrombectomy in total sfa occlusion. Turk J Vasc Surg. Published online November 27, 2024.
Vargas, A. G. D., Montero, N. E., Guerra, P. H., Almeida, R. M. D., Santana, I. E. R., et al. (2025). Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. International Journal of Cardiovascular and Thoracic Surgery, 11(1), 1-5. https://doi.org/10.11648/j.ijcts.20251101.11
Vargas, A. G. D.; Montero, N. E.; Guerra, P. H.; Almeida, R. M. D.; Santana, I. E. R., et al. Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. Int. J. Cardiovasc. Thorac. Surg.2025, 11(1), 1-5. doi: 10.11648/j.ijcts.20251101.11
Vargas AGD, Montero NE, Guerra PH, Almeida RMD, Santana IER, et al. Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. Int J Cardiovasc Thorac Surg. 2025;11(1):1-5. doi: 10.11648/j.ijcts.20251101.11
@article{10.11648/j.ijcts.20251101.11,
author = {Antonio García de Vargas and Noelia Elías Montero and Pedro Hernández Guerra and Rui Mouta de Almeida and Isaura Elena Rodríguez Santana and Pedro Airám Betancor Heredia},
title = {Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {1},
pages = {1-5},
doi = {10.11648/j.ijcts.20251101.11},
url = {https://doi.org/10.11648/j.ijcts.20251101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251101.11},
abstract = {One of the main therapeutic options for the treatment of peripheral arterial disease is endovascular treatment, which has proven to be an effective and less invasive alternative to open surgery. This approach offers several advantages, such as faster recovery and a shorter hospital stay. However, it can also lead to complications, including restenosis and in-stent occlusion, which can compromise the effectiveness of the procedure and have a negative impact on patients' quality of life. Faced with this problem, innovative solutions have emerged, such as rotational atherectomy with the BYCROSS® device, which has positioned itself as a promising tool for the treatment of complex arterial lesions and in-stent thrombosis. This device allows controlled removal of obstructive material, optimizes blood flow and improves short- and long-term outcomes. In this case report, we present a patient with a history of peripheral arterial disease who developed in-stent thrombosis, a common but difficult complication associated with previous endovascular treatments. The patient was successfully treated with rotational atherectomy using the BYCROSS® device, achieving excellent angiographic and clinical results. Subsequently, a significant improvement in symptoms and quality of life was observed. This case highlights the importance of innovative technologies in current clinical practice and the need for a comprehensive and personalized approach in the treatment of vascular complications in patients with peripheral arterial disease.
},
year = {2025}
}
TY - JOUR
T1 - Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease
AU - Antonio García de Vargas
AU - Noelia Elías Montero
AU - Pedro Hernández Guerra
AU - Rui Mouta de Almeida
AU - Isaura Elena Rodríguez Santana
AU - Pedro Airám Betancor Heredia
Y1 - 2025/01/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251101.11
DO - 10.11648/j.ijcts.20251101.11
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 1
EP - 5
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251101.11
AB - One of the main therapeutic options for the treatment of peripheral arterial disease is endovascular treatment, which has proven to be an effective and less invasive alternative to open surgery. This approach offers several advantages, such as faster recovery and a shorter hospital stay. However, it can also lead to complications, including restenosis and in-stent occlusion, which can compromise the effectiveness of the procedure and have a negative impact on patients' quality of life. Faced with this problem, innovative solutions have emerged, such as rotational atherectomy with the BYCROSS® device, which has positioned itself as a promising tool for the treatment of complex arterial lesions and in-stent thrombosis. This device allows controlled removal of obstructive material, optimizes blood flow and improves short- and long-term outcomes. In this case report, we present a patient with a history of peripheral arterial disease who developed in-stent thrombosis, a common but difficult complication associated with previous endovascular treatments. The patient was successfully treated with rotational atherectomy using the BYCROSS® device, achieving excellent angiographic and clinical results. Subsequently, a significant improvement in symptoms and quality of life was observed. This case highlights the importance of innovative technologies in current clinical practice and the need for a comprehensive and personalized approach in the treatment of vascular complications in patients with peripheral arterial disease.
VL - 11
IS - 1
ER -
Vargas, A. G. D., Montero, N. E., Guerra, P. H., Almeida, R. M. D., Santana, I. E. R., et al. (2025). Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. International Journal of Cardiovascular and Thoracic Surgery, 11(1), 1-5. https://doi.org/10.11648/j.ijcts.20251101.11
Vargas, A. G. D.; Montero, N. E.; Guerra, P. H.; Almeida, R. M. D.; Santana, I. E. R., et al. Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. Int. J. Cardiovasc. Thorac. Surg.2025, 11(1), 1-5. doi: 10.11648/j.ijcts.20251101.11
Vargas AGD, Montero NE, Guerra PH, Almeida RMD, Santana IER, et al. Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease. Int J Cardiovasc Thorac Surg. 2025;11(1):1-5. doi: 10.11648/j.ijcts.20251101.11
@article{10.11648/j.ijcts.20251101.11,
author = {Antonio García de Vargas and Noelia Elías Montero and Pedro Hernández Guerra and Rui Mouta de Almeida and Isaura Elena Rodríguez Santana and Pedro Airám Betancor Heredia},
title = {Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {1},
pages = {1-5},
doi = {10.11648/j.ijcts.20251101.11},
url = {https://doi.org/10.11648/j.ijcts.20251101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251101.11},
abstract = {One of the main therapeutic options for the treatment of peripheral arterial disease is endovascular treatment, which has proven to be an effective and less invasive alternative to open surgery. This approach offers several advantages, such as faster recovery and a shorter hospital stay. However, it can also lead to complications, including restenosis and in-stent occlusion, which can compromise the effectiveness of the procedure and have a negative impact on patients' quality of life. Faced with this problem, innovative solutions have emerged, such as rotational atherectomy with the BYCROSS® device, which has positioned itself as a promising tool for the treatment of complex arterial lesions and in-stent thrombosis. This device allows controlled removal of obstructive material, optimizes blood flow and improves short- and long-term outcomes. In this case report, we present a patient with a history of peripheral arterial disease who developed in-stent thrombosis, a common but difficult complication associated with previous endovascular treatments. The patient was successfully treated with rotational atherectomy using the BYCROSS® device, achieving excellent angiographic and clinical results. Subsequently, a significant improvement in symptoms and quality of life was observed. This case highlights the importance of innovative technologies in current clinical practice and the need for a comprehensive and personalized approach in the treatment of vascular complications in patients with peripheral arterial disease.
},
year = {2025}
}
TY - JOUR
T1 - Use of the BYCROSS® Device for the Treatment of Stent Thrombosis as a Complication of Endovascular Treatment of Peripheral Artery Disease
AU - Antonio García de Vargas
AU - Noelia Elías Montero
AU - Pedro Hernández Guerra
AU - Rui Mouta de Almeida
AU - Isaura Elena Rodríguez Santana
AU - Pedro Airám Betancor Heredia
Y1 - 2025/01/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251101.11
DO - 10.11648/j.ijcts.20251101.11
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 1
EP - 5
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251101.11
AB - One of the main therapeutic options for the treatment of peripheral arterial disease is endovascular treatment, which has proven to be an effective and less invasive alternative to open surgery. This approach offers several advantages, such as faster recovery and a shorter hospital stay. However, it can also lead to complications, including restenosis and in-stent occlusion, which can compromise the effectiveness of the procedure and have a negative impact on patients' quality of life. Faced with this problem, innovative solutions have emerged, such as rotational atherectomy with the BYCROSS® device, which has positioned itself as a promising tool for the treatment of complex arterial lesions and in-stent thrombosis. This device allows controlled removal of obstructive material, optimizes blood flow and improves short- and long-term outcomes. In this case report, we present a patient with a history of peripheral arterial disease who developed in-stent thrombosis, a common but difficult complication associated with previous endovascular treatments. The patient was successfully treated with rotational atherectomy using the BYCROSS® device, achieving excellent angiographic and clinical results. Subsequently, a significant improvement in symptoms and quality of life was observed. This case highlights the importance of innovative technologies in current clinical practice and the need for a comprehensive and personalized approach in the treatment of vascular complications in patients with peripheral arterial disease.
VL - 11
IS - 1
ER -