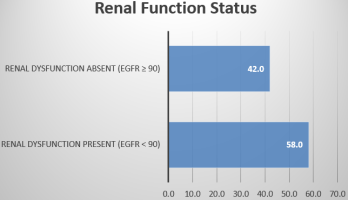
Chronic heart failure is a major global health problem associated with substantial morbidity and mortality, and its close interaction with renal function through the cardiorenal syndrome significantly influences disease progression and outcomes. Renal dysfunction is commonly encountered in patients with chronic heart failure and is known to be associated with adverse prognosis; however, its burden in routine clinical settings, particularly in local populations, remains insufficiently characterized. The purpose of this study was to determine the prevalence of renal dysfunction among patients with chronic heart failure and to examine its association with key clinical variables. To achieve this, a hospital-based cross-sectional study was conducted in the Department of Cardiology at Satkhira Medical College and Hospital, Bangladesh, including 150 patients diagnosed with chronic heart failure. Relevant demographic and clinical data were collected, and renal function was assessed using estimated glomerular filtration rate calculated by the CKD-EPI equation. Statistical analysis was performed to evaluate the relationship between renal dysfunction and selected variables. The findings demonstrated that renal dysfunction was present in 58.0% of patients, with moderate impairment being the most common pattern, and was significantly associated with older age, hypertension, diabetes mellitus, and advanced NYHA functional class. In conclusion, this study highlights the substantial burden of renal dysfunction among patients with chronic heart failure and emphasizes the importance of routine renal function assessment for early identification and improved clinical management in this high-risk population.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 12, Issue 3) |
| DOI | 10.11648/j.ijcts.20261203.12 |
| Page(s) | 92-98 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Chronic Heart Failure, Renal Dysfunction, Prevalence, Cardiorenal Syndrome, Glomerular Filtration Rate
Variable | Frequency (n) | Percentage (%) | |
|---|---|---|---|
Age Group (years) | ≤40 | 28 | 18.7 |
41–50 | 32 | 21.3 | |
51–70 | 70 | 46.7 | |
>70 | 20 | 13.3 | |
Mean Age (years) | 55.4 ± 11.3 | ||
Sex | Male | 92 | 61.3 |
Female | 58 | 38.7 | |
Comorbidities | Hypertension | 102 | 68.0 |
Diabetes Mellitus | 76 | 50.7 | |
Etiology of Heart Failure | Ischemic Heart Disease | 88 | 58.7 |
Non-ischemic Causes | 62 | 41.3 | |
eGFR Category (mL/min/1.73 m2) | Severity | Frequency (n) | Percentage (%) |
|---|---|---|---|
≥90 | Normal | 63 | 42.0 |
60–89 | Mild Dysfunction | 28 | 18.7 |
30–59 | Moderate Dysfunction | 41 | 27.3 |
<30 | Severe Dysfunction | 18 | 12.0 |
Variable | Renal Dysfunction Present n (%) | Renal Dysfunction Absent n (%) | p-value |
|---|---|---|---|
Age ≥60 years | 54 (67.5) | 26 (32.5) | 0.020 |
Hypertension | 68 (66.7) | 34 (33.3) | 0.001 |
Diabetes Mellitus | 52 (68.4) | 24 (31.6) | 0.030 |
NYHA Class III–IV | 57 (65.5) | 30 (34.5) | 0.004 |
NYHA Class I–II | 30 (42.3) | 33 (57.7) | - |
CHF | Chronic Heart Failure |
CKD | Chronic Kidney Disease |
CKD EPI | Chronic Kidney Disease Epidemiology Collaboration |
CRS | Cardiorenal Syndrome |
eGFR | Estimated Glomerular Filtration Rate |
GFR | Glomerular Filtration Rate |
IBM | International Business Machines Corporation |
NYHA | New York Heart Association |
RD | Renal Dysfunction |
SPSS | Statistical Package for the Social Sciences |
WRF | Worsening Renal Function |
| [1] | Braunwald E. The war against heart failure: the Lancet lecture. The Lancet. 2015 Feb 28; 385(9970): 812-24. |
| [2] | Cowie MR, Mosterd A, Wood D, Deckers JW, Poole-Wilson PA, Sutton G, Grobbee D. The epidemiology of heart failure. European heart journal. 1997 Feb 1; 18(2): 208-25. |
| [3] | Ronco C, McCullough PA, Anker SD, Anand I, Aspromonte N, Bagshaw SM, Bellomo R, Berl T, Bobek I, Cruz DN, Daliento L. Cardiorenal syndromes: an executive summary from the consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contributions to nephrology. 2010 Apr 20; 165: 54-67. |
| [4] | Kamilova U, Abdullaeva C, Zakirova G, Masharipova D, Tagaeva D. Assessment of Kidney Dysfunction in Patients with Chronic Heart Failure. Open Access Macedonian Journal of Medical Sciences. 2022 Sep 10; 10(B): 2093-7. |
| [5] | de Silva R, Nikitin NP, Witte KK, Rigby AS, Goode K, Bhandari S, Clark AL, Cleland JG. Incidence of renal dysfunction over 6 months in patients with chronic heart failure due to left ventricular systolic dysfunction: contributing factors and relationship to prognosis. European heart journal. 2006 Mar 1; 27(5): 569-81. |
| [6] | McMurray JJ, Östergren J, Swedberg K, Granger CB, Held P, Michelson EL, Olofsson B, Yusuf S, Pfeffer MA. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. The Lancet. 2003 Sep 6; 362(9386): 767-71. |
| [7] | SOLVD Investigators*. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. New England Journal of Medicine. 1992 Sep 3; 327(10): 685-91. |
| [8] | Solomon SD, Wang D, Finn P, Skali H, Zornoff L, McMurray JJ, Swedberg K, Yusuf S, Granger CB, Michelson EL, Pocock S. Effect of candesartan on cause-specific mortality in heart failure patients: the Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation. 2004 Oct 12; 110(15): 2180-3. |
| [9] | Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B. Eplerenone in patients with systolic heart failure and mild symptoms. New England Journal of Medicine. 2011 Jan 6; 364(1): 11-21. |
| [10] | Cleland JG, Carubelli V, Castiello T, Yassin A, Pellicori P, Antony R. Renal dysfunction in acute and chronic heart failure: prevalence, incidence and prognosis. Heart failure reviews. 2012 Mar; 17(2): 133-49. |
| [11] | Costanzo MR. The cardiorenal syndrome in heart failure. Heart failure clinics. 2020 Jan 1; 16(1): 81-97. |
| [12] | Cowie MR, Komajda M, Murray-Thomas T, Underwood J, Ticho B. Prevalence and impact of worsening renal function in patients hospitalized with decompensated heart failure: results of the prospective outcomes study in heart failure (POSH). European Heart Journal. 2006 May 1; 27(10): 1216-22. |
| [13] | Klein L, Massie BM, Leimberger JD, O’Connor CM, Piña IL, Adams Jr KF, Califf RM, Gheorghiade M. Admission or changes in renal function during hospitalization for worsening heart failure predict postdischarge survival: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF). Circulation: Heart Failure. 2008 May 1; 1(1): 25-33. |
| [14] | Giamouzis G, Kalogeropoulos A, Georgiopoulou V, Laskar S, Smith AL, Dunbar S, Triposkiadis F, Butler J. Hospitalization epidemic in patients with heart failure: risk factors, risk prediction, knowledge gaps, and future directions. Journal of cardiac failure. 2011 Jan 1; 17(1): 54-75. |
| [15] | Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, Krumholz HM. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. Journal of the American College of Cardiology. 2006 May 16; 47(10): 1987-96. |
| [16] | McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal insufficiency and heart failure: prognostic and therapeutic implications from a prospective cohort study. Circulation. 2004 Mar 2; 109(8): 1004-9. |
| [17] | Metra M, Cotter G, Gheorghiade M, Dei Cas L, Voors AA. The role of the kidney in heart failure. European heart journal. 2012 Sep 1; 33(17): 2135-42. |
| [18] | Fonarow GC, Abraham WT, Albert NM, Stough WG, Gheorghiade M, Greenberg BH, O’Connor CM, Pieper K, Sun JL, Yancy CW, Young JB. Influence of a performance-improvement initiative on quality of care for patients hospitalized with heart failure: results of the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure (OPTIMIZE-HF). Archives of internal medicine. 2007 Jul 23; 167(14): 1493-502. |
| [19] | Heywood JT, Fonarow GC, Costanzo MR, et al. High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heart failure: a report from the ADHERE database. J Card Fail 2007; 13: 422–30. |
| [20] | Jeele MO, Hussein AA, Mohamud MA, Adani AA, Mohamud MF. Spectrum and prevalence of renal dysfunction among heart failure patients attending tertiary care hospital: first report from Somalia. The Egyptian Journal of Internal Medicine. 2023 Oct 5; 35(1): 70. |
| [21] | Levin A, Foley RN. Cardiovascular disease in chronic renal insufficiency. American journal of kidney diseases. 2000 Dec 1; 36(6): S24-30. |
| [22] | Packer M, Carver JR, Rodeheffer RJ, Ivanhoe RJ, DiBianco R, Zeldis SM, Hendrix GH, Bommer WJ, Elkayam U, Kukin ML, Mallis GI. Effect of oral milrinone on mortality in severe chronic heart failure. New England Journal of Medicine. 1991 Nov 21; 325(21): 1468-75. |
| [23] | Forman DE, Butler J, Wang Y, Abraham WT, O'Connor CM, Gottlieb SS, Loh E, Massie BM, Rich MW, Stevenson LW, Young JB. Incidence, predictors at admission, and impact of worsening renal function among patients hospitalized with heart failure. Journal of the American College of Cardiology. 2004 Jan 7; 43(1): 61-7. |
| [24] | Bibbins-Domingo K, Lin F, Vittinghoff E, Barrett-Connor E, Grady D, Shlipak MG. Renal insufficiency as an independent predictor of mortality among women with heart failure. Journal of the American College of Cardiology. 2004 Oct 19; 44(8): 1593-600. |
| [25] | Ahmed A, Campbell RC. Epidemiology of chronic kidney disease in heart failure. Heart Fail Clin. 2008 Oct; 4(4): 387-99. |
| [26] | Shen X, Guo H, Mantica G, Yuan H. Analysis of the clinical features and risk factors of kidney injury in patients with chronic heart failure—a retrospective cohort study. Journal of Thoracic Disease. 2023 Jul 25; 15(7): 3934. |
| [27] | Löfman I, Szummer K, Hagerman I, Dahlström U, Lund LH, Jernberg T. Prevalence and prognostic impact of kidney disease on heart failure patients. Open Heart. 2016 Jan 18; 3(1): e000324. |
| [28] | Lawson CA, Testani JM, Mamas M, Damman K, Jones PW, Teece L, Kadam UT. Chronic kidney disease, worsening renal function and outcomes in a heart failure community setting: A UK national study. Int J Cardiol. 2018 Sep 15; 267: 120-127. |
| [29] | Cobo Marcos M, de la Espriella R, Gayán Ordás J, Llàcer P, Pomares A, Fort A, Ponz de Antonio I, Méndez A, Blázquez-Bermejo Z, Caravaca Pérez P, Rubio Gracia J, Recio-Mayoral A, Zegrí I, García Pinilla JM, Montero Hernández E, Castro A, Soler MJ, Górriz JL, Bascompte Claret R, Fluvià-Brugués P, Manzano L, Núñez J. Prevalence and clinical profile of kidney disease in patients with chronic heart failure. Insights from the Spanish cardiorenal registry. Rev Esp Cardiol (Engl Ed). 2024 Jan; 77(1): 50-59. |
| [30] | Stanojević D, Apostolović S, Janković-Tomasević R, Salinger-Martinović S, Pavlović M, Zivković M, Bozinović N, Kutlesić-Kurtović D. Prevalence of renal dysfunction and its influence on functional capacity in elderly patients with stable chronic heart failure. Vojnosanit Pregl. 2012 Oct; 69(10): 840-5. |
| [31] | Beck H, Titze SI, Hübner S, Busch M, Schlieper G, Schultheiss UT, Wanner C, Kronenberg F, Krane V, Eckardt KU, Köttgen A; GCKD Investigators. Heart failure in a cohort of patients with chronic kidney disease: the GCKD study. PLoS One. 2015 Apr 13; 10(4): e0122552. |
| [32] | Li J, Chu Y, Huang M. Impact of renal dysfunction on prognosis in patients with severe heart failure: A retrospective cohort study. Medicine (Baltimore). 2025 Oct 10; 104(41): e44405. |
| [33] | Zhang H, Shi S, Zhao XJ, Wang JK, Liu ZW, Liu FQ, Zhu L, Zhu SM, Zhang Y, Pan S. Association between the lipid profile and renal dysfunction in the heart failure patients. Kidney and Blood Pressure Research. 2019 Feb 22; 44(1): 52-61. |
| [34] | Galil AG, Pinheiro HS, Chaoubah A, Costa DM, Bastos MG. Chronic kidney disease increases cardiovascular unfavourable outcomes in outpatients with heart failure. BMC nephrology. 2009 Oct 21; 10(1): 31. |
APA Style
Das, S. K., Das, R., Karmoker, K. K., Alam, N. (2026). Prevalence of Renal Dysfunction Among Patients with Chronic Heart Failure. International Journal of Cardiovascular and Thoracic Surgery, 12(3), 92-98. https://doi.org/10.11648/j.ijcts.20261203.12
ACS Style
Das, S. K.; Das, R.; Karmoker, K. K.; Alam, N. Prevalence of Renal Dysfunction Among Patients with Chronic Heart Failure. Int. J. Cardiovasc. Thorac. Surg. 2026, 12(3), 92-98. doi: 10.11648/j.ijcts.20261203.12
@article{10.11648/j.ijcts.20261203.12,
author = {Suman Kumar Das and Reba Das and Kajal Kumar Karmoker and Nur Alam},
title = {Prevalence of Renal Dysfunction Among Patients with Chronic Heart Failure},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {3},
pages = {92-98},
doi = {10.11648/j.ijcts.20261203.12},
url = {https://doi.org/10.11648/j.ijcts.20261203.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261203.12},
abstract = {Chronic heart failure is a major global health problem associated with substantial morbidity and mortality, and its close interaction with renal function through the cardiorenal syndrome significantly influences disease progression and outcomes. Renal dysfunction is commonly encountered in patients with chronic heart failure and is known to be associated with adverse prognosis; however, its burden in routine clinical settings, particularly in local populations, remains insufficiently characterized. The purpose of this study was to determine the prevalence of renal dysfunction among patients with chronic heart failure and to examine its association with key clinical variables. To achieve this, a hospital-based cross-sectional study was conducted in the Department of Cardiology at Satkhira Medical College and Hospital, Bangladesh, including 150 patients diagnosed with chronic heart failure. Relevant demographic and clinical data were collected, and renal function was assessed using estimated glomerular filtration rate calculated by the CKD-EPI equation. Statistical analysis was performed to evaluate the relationship between renal dysfunction and selected variables. The findings demonstrated that renal dysfunction was present in 58.0% of patients, with moderate impairment being the most common pattern, and was significantly associated with older age, hypertension, diabetes mellitus, and advanced NYHA functional class. In conclusion, this study highlights the substantial burden of renal dysfunction among patients with chronic heart failure and emphasizes the importance of routine renal function assessment for early identification and improved clinical management in this high-risk population.},
year = {2026}
}
TY - JOUR T1 - Prevalence of Renal Dysfunction Among Patients with Chronic Heart Failure AU - Suman Kumar Das AU - Reba Das AU - Kajal Kumar Karmoker AU - Nur Alam Y1 - 2026/04/30 PY - 2026 N1 - https://doi.org/10.11648/j.ijcts.20261203.12 DO - 10.11648/j.ijcts.20261203.12 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 92 EP - 98 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20261203.12 AB - Chronic heart failure is a major global health problem associated with substantial morbidity and mortality, and its close interaction with renal function through the cardiorenal syndrome significantly influences disease progression and outcomes. Renal dysfunction is commonly encountered in patients with chronic heart failure and is known to be associated with adverse prognosis; however, its burden in routine clinical settings, particularly in local populations, remains insufficiently characterized. The purpose of this study was to determine the prevalence of renal dysfunction among patients with chronic heart failure and to examine its association with key clinical variables. To achieve this, a hospital-based cross-sectional study was conducted in the Department of Cardiology at Satkhira Medical College and Hospital, Bangladesh, including 150 patients diagnosed with chronic heart failure. Relevant demographic and clinical data were collected, and renal function was assessed using estimated glomerular filtration rate calculated by the CKD-EPI equation. Statistical analysis was performed to evaluate the relationship between renal dysfunction and selected variables. The findings demonstrated that renal dysfunction was present in 58.0% of patients, with moderate impairment being the most common pattern, and was significantly associated with older age, hypertension, diabetes mellitus, and advanced NYHA functional class. In conclusion, this study highlights the substantial burden of renal dysfunction among patients with chronic heart failure and emphasizes the importance of routine renal function assessment for early identification and improved clinical management in this high-risk population. VL - 12 IS - 3 ER -
Department of Cardiology, Satkhira Medical College Hospital, Satkhira, Bangladesh
Department of Pathology, Satkhira Medical College, Satkhira, Bangladesh
Department of Cardiology, Faridpur Medical College, Faridpur, Bangladesh
Department of Cardiology, Satkhira Medical College, Satkhira, Bangladesh
Information